GI Endoscopy · 12 min read
Recap: Live Chat Over the Scope Clip

MEMBER ARTICLE
Below is the full transcript from our discussion on Over the Scope Clip on April 17, 2021.
[membership level="0"]Continue with EndoCollab membership.
Get the full article plus the complete EndoCollab library of courses, cases, classifications, and practical teaching resources.
Below is the full transcript from our discussion on Over the Scope Clip on April 17, 2021.

This chat will be available as an article for you to review, and of course to ask more questions in EndoCollab after it is finished.

Hi All. I have done 3-4 of these for bleeding. I would like to know a couple of practical tips I.e. do you simply press over the vessel? Tap suck the vessel into the cap like a varix or even pull the ulcer base into your cap with graspers?
As part of the Post-Graduate Course "From My Toolbox: Tips and Tricks for GI Endoscopy, will have three lectures on OTSC in the future. Stay tuned for updates.
Let's begin! :)

Hi everybody, welcome
I have started to answer one questions. Here we go.


Now some basics on the clips with the first question.
1. Hi, I want to know how do you decide the size and the type of the Ovesco? For example, fistulas? Bleeding ulcers or gastric lesions...?
The main factors are size of defect, location, angulation and consistency of tissue. The size of OTSC ids categorized based on the cap it comes with. The cap is essential for entrapping the tissue. The cap diameter may vary from 11 to 14 mm. And the cap length may be 3 to 6 mm. In addition, the “teeth” of the OTSC may be sharp (named “t” for therapeutic) or blunted (“a” for atraumatic”). The sharp teeth are better for grasping tissue tightly. I prefer those. I don´t use much “a” OTSC anymore. So, based on diameter,cap length and teeth, the OTSC is classified as 11/6t, 11/6a, 12/3a, etc. A 12/6t is 12 mm diameter, 6 mm distal cap (more tissue grasping) and has sharp teeth (“t” for therapeutic).
The main factors are size of defect, location, angulation and consistency of tissue. The size of OTSC ids categorized based on the cap it comes with. The cap is essential for entrapping the tissue. The cap diameter may vary from 11 to 14 mm. And the cap length may be 3 to 6 mm. In addition, the “teeth” of the OTSC may be sharp (named “t” for therapeutic) or blunted (“a” for atraumatic”). The sharp teeth are better for grasping tissue tightly. I prefer those. I don´t use much “a” OTSC anymore. So, based on diameter,cap length and teeth, the OTSC is classified as 11/6t, 11/6a, 12/3a, etc. A 12/6t is 12 mm diameter, 6 mm distal cap (more tissue grasping) and has sharp teeth (“t” for therapeutic).

It is essential to understand the shape, diameter and tip of the cap where the OTSC is loaded onto.
The diameter and distal end are essential for you to decide on the size of defects that can be closed and amount of tissue to be engulfed inside. The best upper GI OTSC is the 12/6t. The 14/6t is for colon use. The 11/6t is good for patients with smaller diameter esophagus lumen (elderly, young patients)
Here I show you a picture with the OTSC (and its cap) and other caps we use in endoscopy

Next question
2. Also mucosa around defect how it can decide to apply Ovesco
Usually, the mucosa in bleeding ulcers or perforations already has exposed vessels and stroma and thus should be ideal for healing once apposed. However, long standing fistulae may have normal mucosa. Therefore, we like to biopsy borders or apply argon plasma coagulation to get some “live” tissue activity.
Usually, the mucosa in bleeding ulcers or perforations already has exposed vessels and stroma and thus should be ideal for healing once apposed. However, long standing fistulae may have normal mucosa. Therefore, we like to biopsy borders or apply argon plasma coagulation to get some “live” tissue activity.


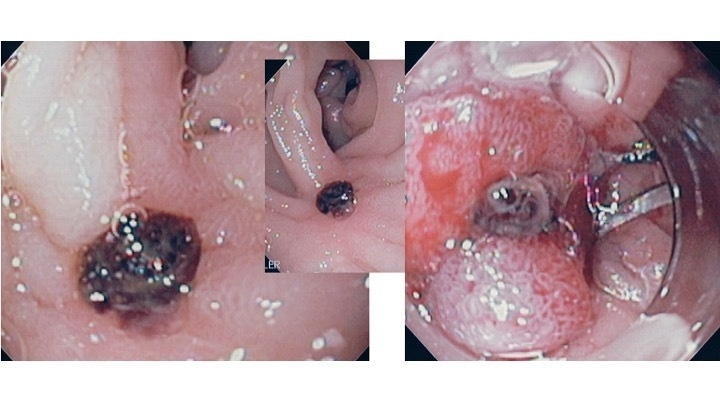
“GC” is gastric closure and the teeth are incredibly sharp.
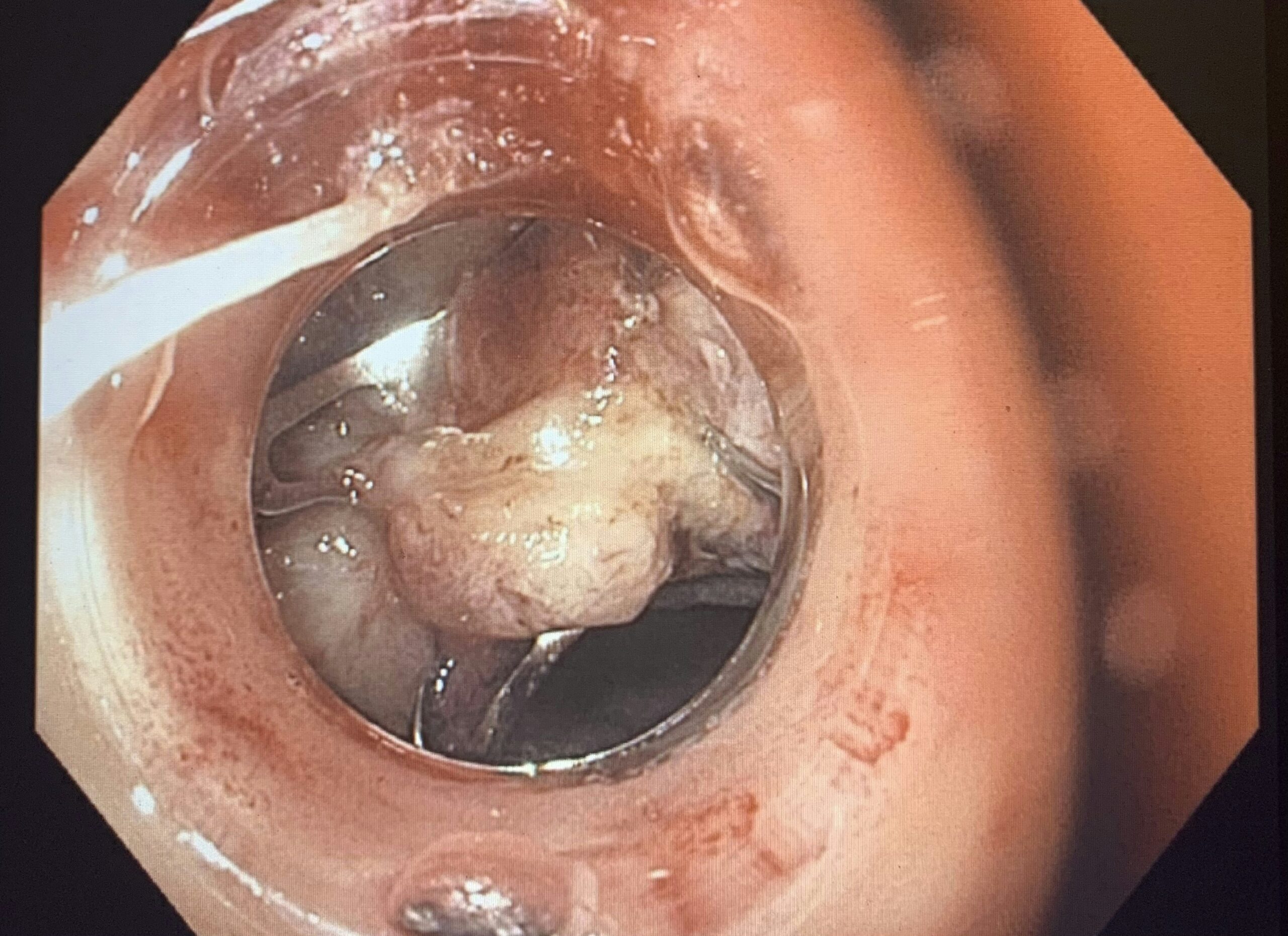
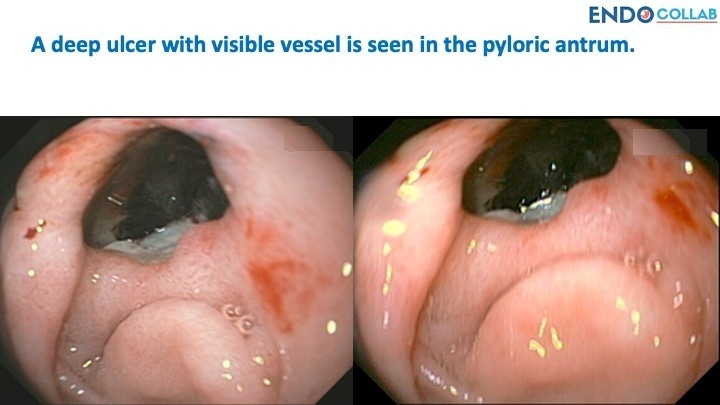
Look at the picture of the bleeding ulcer. The tissue is "active", damaged, with exposure of stroma, fibrin, coagulation factors, small vessels, and of course pro-collagen.
Perfect Andy! The gc the are fantastic. Initially designed for "gastric closure", closure of gastrocutaneous fistulas. They are "t" but sharper. I love those as well.
Your slide is perfect for the next question about closure of gastroecutaneous fistula after PEG removal.
Can Ovesco be applied to to close gastro-cutaneous fistula as a result of PEG tubes?
Yes, this is a great indication. We recommend to use the 12/6gc OTSC for these situations. An exception are older patients or those with narrowed esophagus, as here the OTSC 12/6gc may be too large to go down the esophagus. We use 11/6t in these cases.
Yes, this is a great indication. We recommend to use the 12/6gc OTSC for these situations. An exception are older patients or those with narrowed esophagus, as here the OTSC 12/6gc may be too large to go down the esophagus. We use 11/6t in these cases.
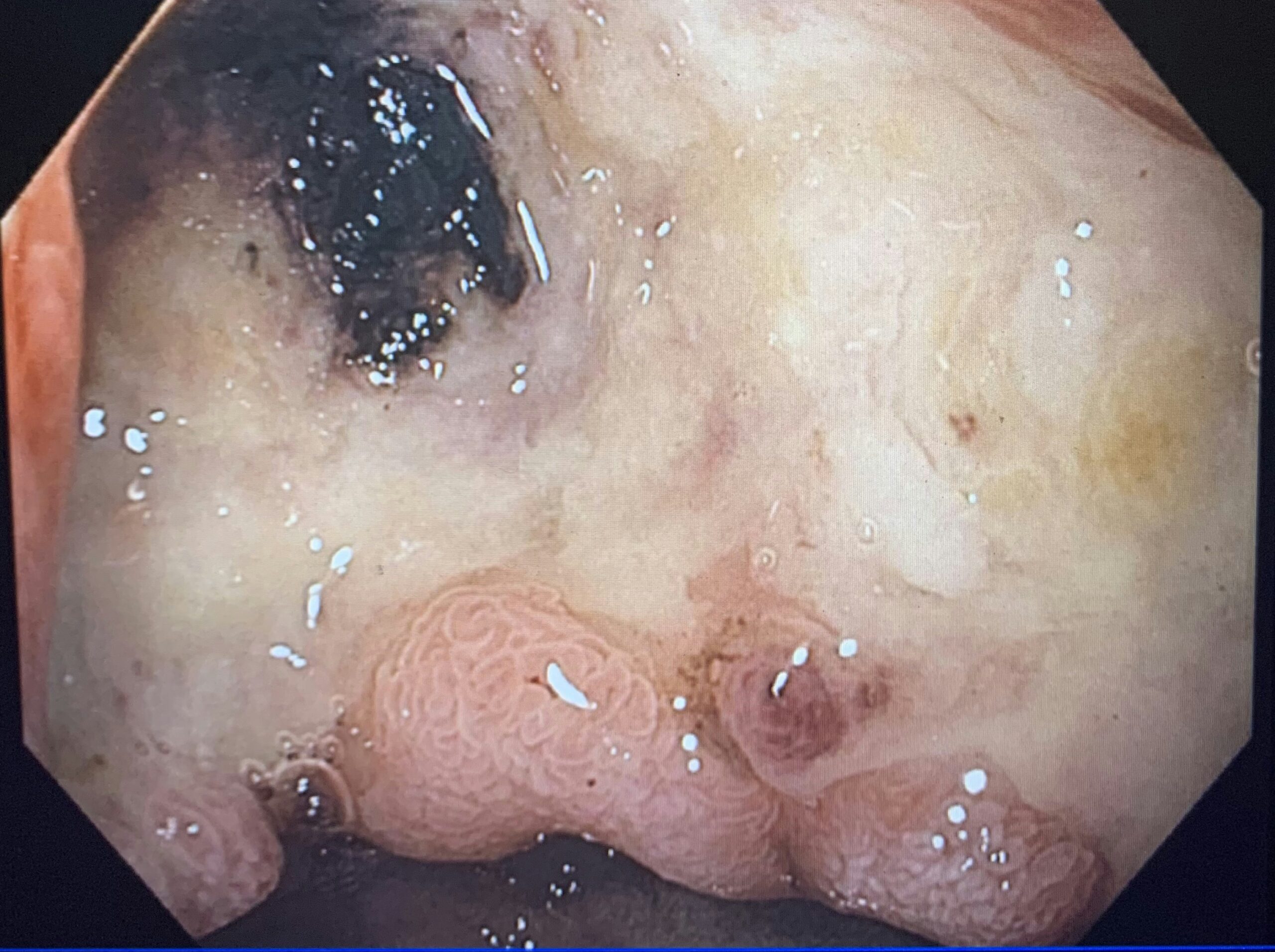
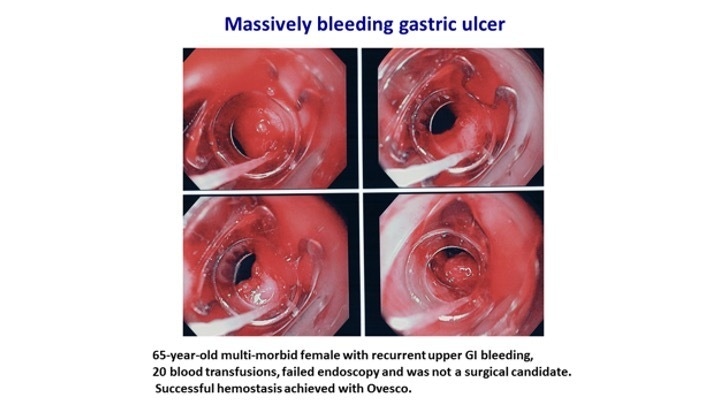
Nice, huge ulcer. In the past, lots of traditional clips were used too treat it. I remember a case using about 10 clips, 5 of which fell off. Now we have OTSC.
Here is an ulcer too large to close, bipolar probe could slip and lead to arterial bleed. This is a nice target for OTSC.
Andy, do you use epinephrine before applying OTSC or do the one-stop-shop? Only Ovesco?
One stop
Excellent case. It shows that one stop is the way to go for those ulcers. Nice!
in don’t want the tissue to get ever denser with Epi injection . Softer better !
The paradigm is changing. The old recommendation of using dual therapy is not valid any more, specifically in these cases
Here another example of OTSC for bleeding ulcer. NO epinephrine used. Just an 12/6t Ovesco
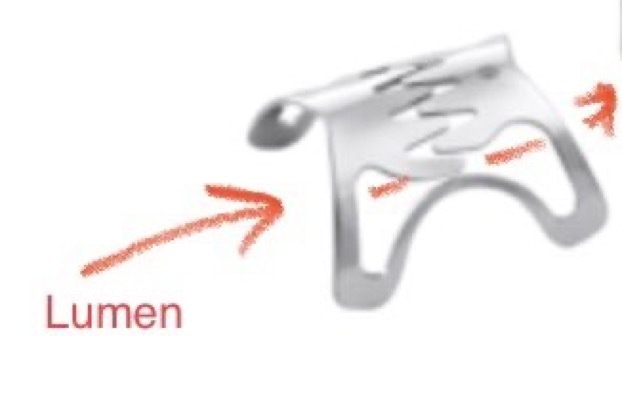
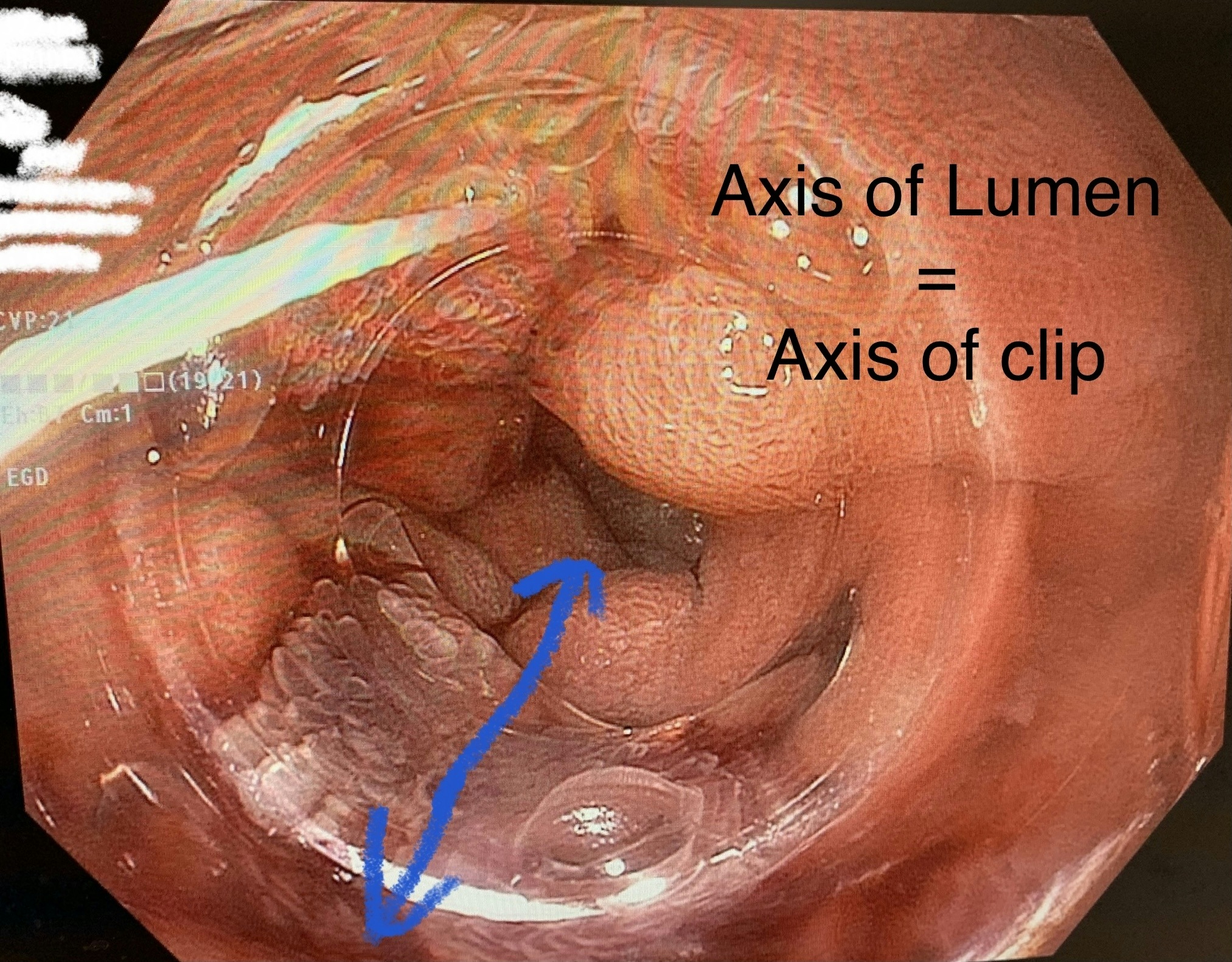
Also remember that the OVESCo OTSC has a directionality to it, like a mouth. So vesse you want to bite vertically not horizontally. Arrange the teeth appropriately!
That vessel** in my image
That's a very important point. You want to have the vessel in the middle of your cap, so it is centered when the clip is released.
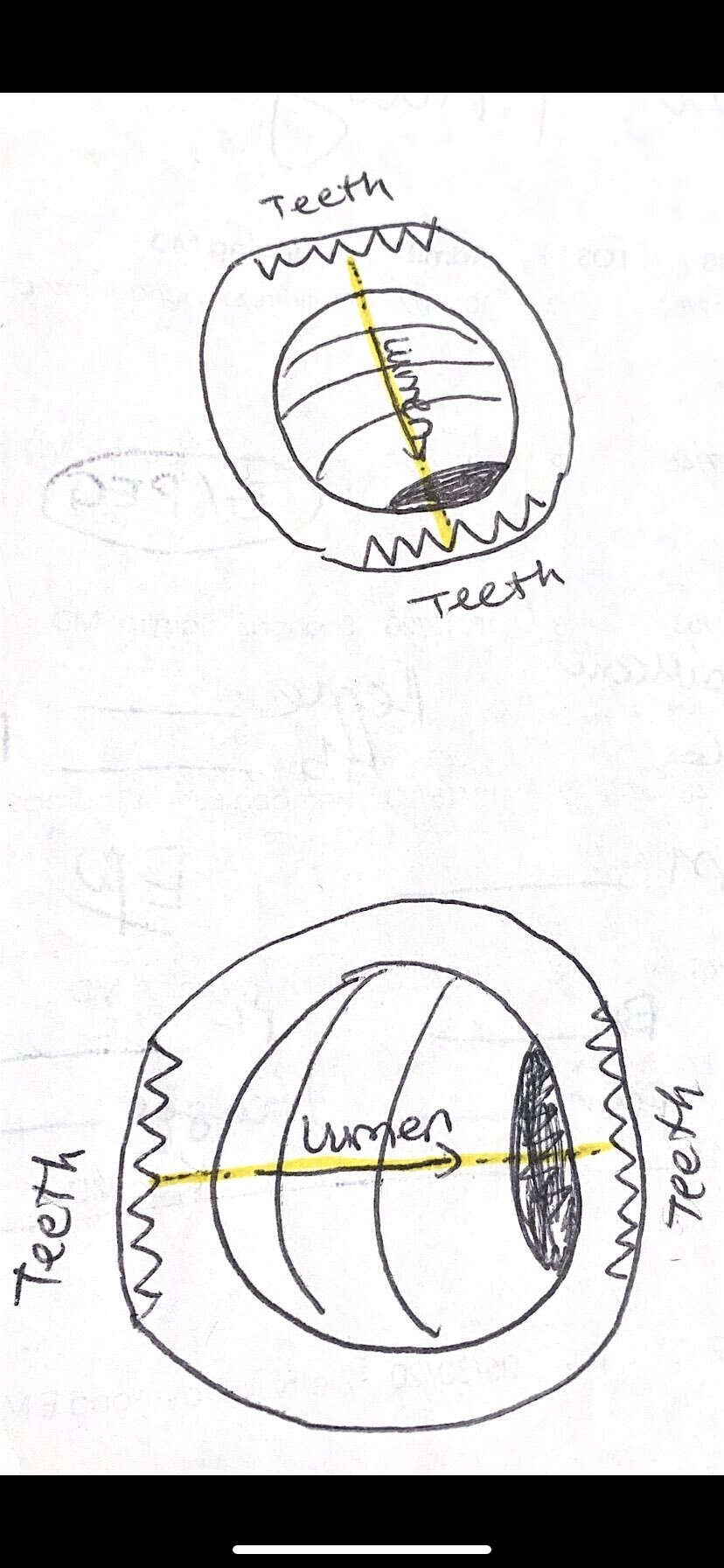
The padlock from Steris has no directionality to it, closing circumferentially. The Ovesco closes along the axis of the teeth.

so how is axis important in OTSC
and what if patient rebleeds after application of OVESCO
can we attempt such patients endoscopically ?
If the vessel is in a huge ulcer, maintaining centrality may not be a problem. However, in ulcers located in the esophagus, lesser curvature, or those ulcers with soft and hard borders, it may be more difficult, as the suction preferentially ingests the soft part and the vessel may be missed.
and can ovesco be used in malignant bleeding ulcers ? like penetrating malignant ulcers with visible vessel ?
The axis pertains to placing the cap "en face", in front of the ulcer with vessel.
can dieulafoy's be clipped with ovesco ?
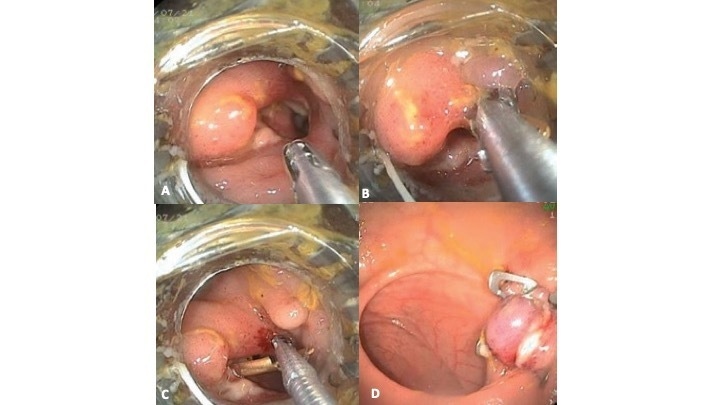
Yes, Dielulafoy can be clipped with Ovesco. Here an example.
Excellent explanation Andy
Question from Dr Evangelos Russo.I would like to know a couple of practical tips I.e. do you simply press over the vessel? Tap suck the vessel into the cap like a varix or even pull the ulcer base into your cap with graspers?
The axis issue is not a big deal in large spaces like stomach, but more important in tight spaces like esophagus and duodenum (sweep). The pillars can obstruct lumen sometimes.
We prefer to face the ulcer/vessel directly, apply some pressure on the ulcer (careful with posterior duodenal ulcers as on my perforate), suction, and release the OTSC
what manoeuvres are helpful in post DU OVESCO application as scope positioning may be difficulty at genu of duodenum
In tight lumens it is important to move the big and small wheels of your scope so you can direct the cap of the clip towards the lesion in an "en face" approach.
Grab more tissue by boosting suction (add vacutainers to suction, therapeutic 1T scope), decompression lumen (underwater even!), not pushing too hard.
Very important, not pushing too hard
add 2 vacutainers “in series “
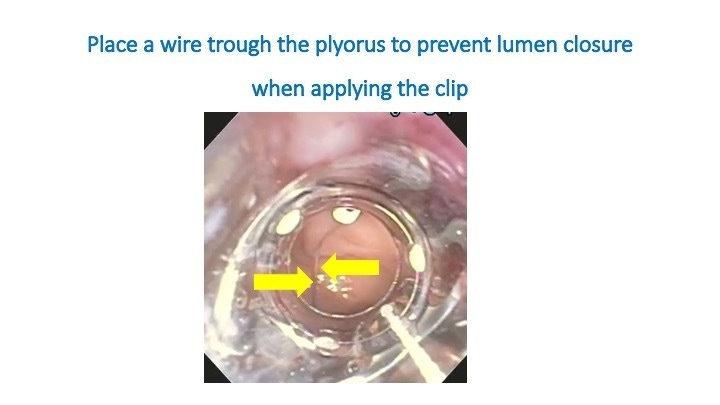
If the ulcer appears ugly and one feels uncomfortable about possible duodenal closure, I like to place a wire first. I advance ability guide wire deep into the upper jejunum, remove the scope and reintroduce next to the wire. The wire always tells me were the lumen is and I apply the OTSC without fear ob the ugly post duodenum ulcer.
Wire doesn’t get stuck?
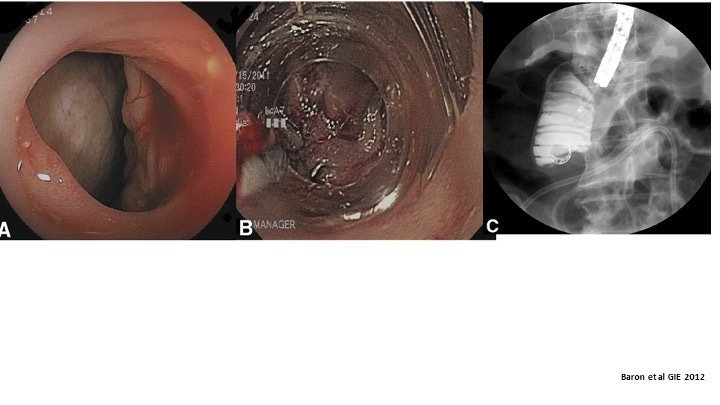
This is a report by Todd Baron of a total duodenal occlusion after he closed a perforation in the duodenum.
This may be avoided by using a wire
oh I see wire is to the the side of scope!
Exactly
so in case we close duodenum with OVESCO is there any endoscopic modality to remove it ?
This is an example of wire place first in the esophagus and into the stomach. This was a case of esophageal fistula. Then I entered again with the scope loaded with the clip. Applied argon plasma coagulation to the fistula, and then deployed the clip. In panel C you can see the wire. The "guiding" wire :)
If you close the duodenum it's a big problem. No way to safely remove it.
I saw once a dispositive for broke the ovesco
with some pulse energy...I saw it on Spain congress
However, if you close the pylorus, it either falls off (because the pylorus moves more and has more force), or you can can carefully snare it off using ESD techniques
can OVESCO cause extraluminal trauma to surrounding viscera ?
As Dr. Hurtado says, there is a dispositive to break down OTSC. It's possible to break with argon plasma coagulation as well, he head generated can be too much and result in perforation. The dispositive is the best option, but it must be present in your unit. We do no have it available in our unit.
Very interesting discussion... thanks to everyone
Yes, Ovesco can entrap viscera. If there is a stomach perforation, you usually entrap omentun. No problem. But in the colon, I you close a perforation, make sure you do not grasp or grab any small bowel. Whatever looks yellow there is NO omentum! Prof. Helmut Neumann has case of small bowel entrapment calling attention to this aspect.
There is an OVESCO Remove system sold, it is a bipolar probe . It’s sold cheaply to encourage more OTSC use.
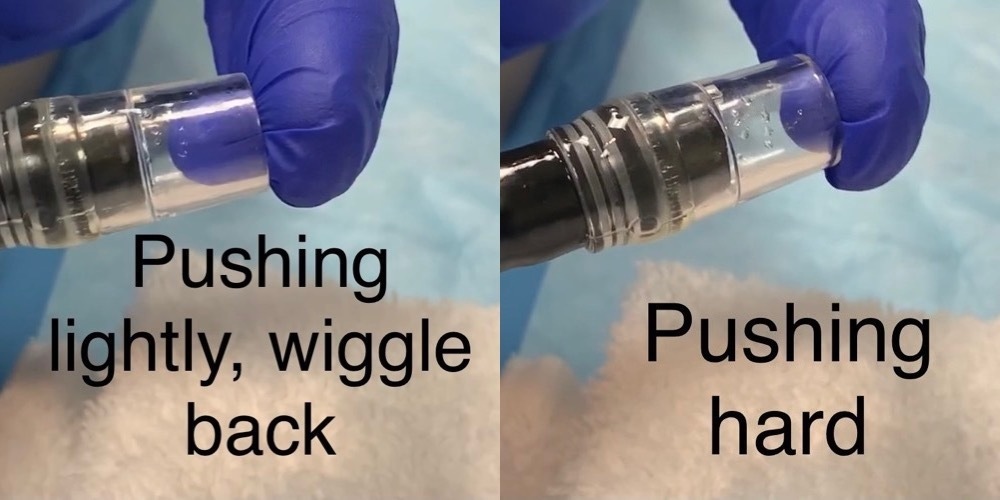
Note you get more tissue with pushing less and having less air in lumen to begin (less wall tension to overcome)
This tip is very important. The aspect of having less air to grasp more tissue. On the side. This is the concept of underwater EMR, you are able to get more tissue as it is in "natural" state, or contracted
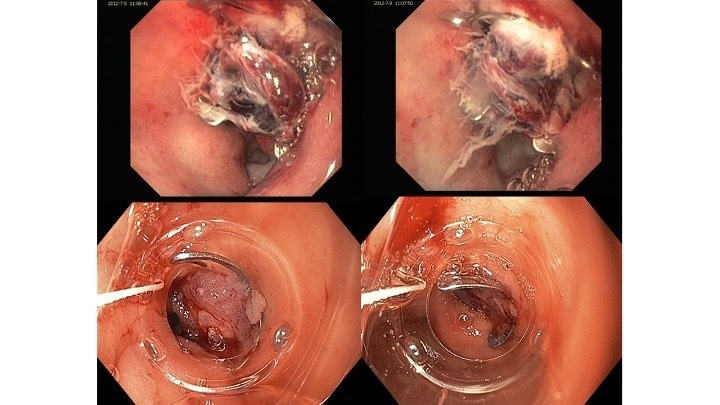
Here another example with wire in patient with huge prepyloric ulcer. I used two clips in this patient.
The pylorus is below
To remove with just APC:
The arrows show the biliary guidewire
Argon steady. Flo rate of 1.2 to 1.5 for more of a straight beam
Absolutely, higher liter flow as you mention.
APC effect 2, 90 watts,
That means, the endoscopist needs to suction more during procedure to prevent overinsufflation
https://onlinelibrary.wiley.com/doi/full/10.1111/den.12925 (APC removal).
Here is another case of using guidewire and nasogastric tube in a patient with esophageal fistula.
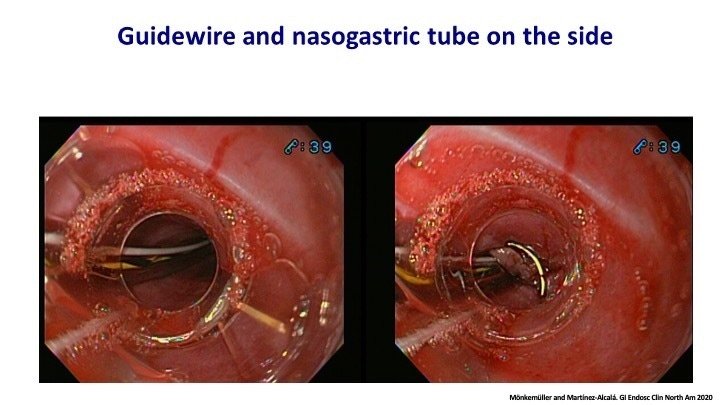
why NGT along with guidewire
In this case the esophagus had previous radiation and by applying the clip I was anticipating stenosis. Therefore, I left the NGT in place for feeding purposes and to serve as a "bridge" for remodeling fibrosis and guarantee a lumen for potential future dlations. The fistula was closed nicely, and the NGT was removed after 5 days. Luckily, without significant stenosis after clip application.
Another question from Dr Jair Morales Alvarado:
any tips to use ovesco in sigmoid perforations?
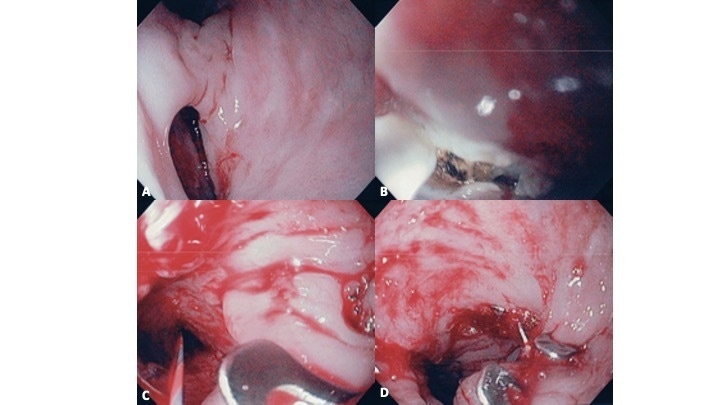
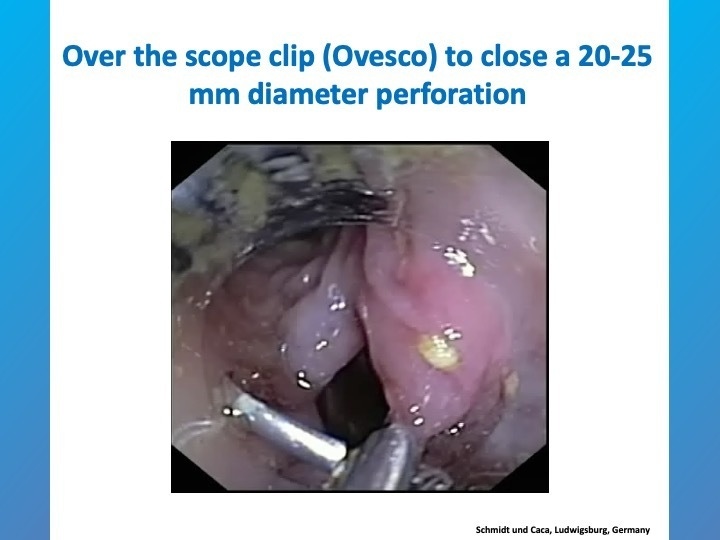
Perforations that are smaller than 20 mm in non-angulated locations may be closed with the "en-face" and suction technique. No need for Twin Grasper.

Small perforation, which could be "suctioned" inside the cap, and the OTSC was released closing it well.
Larger perforations may require the Twin grasper

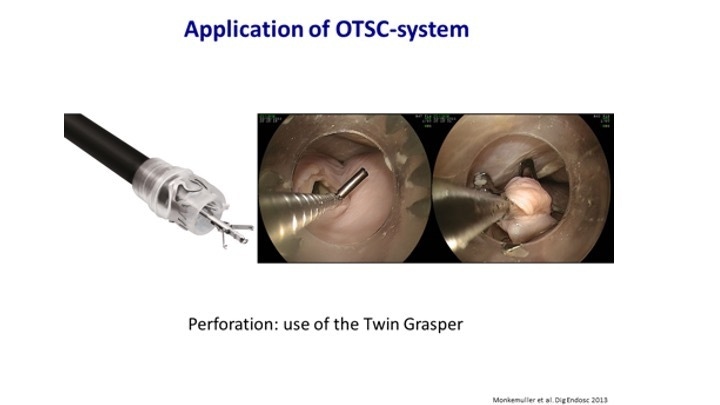
With one arm you grab one edge, close, and open the opposite arm, and go to the contralateral edge, and close the second arm.
Then you start gently pulling, very gently. And at the same time, torquing the tip of the scope. And suctioning. What you want to do is create a "tent" of tissue, which gets located inside of your cap. Once you have this tip or tent or pyramid of tissue inside the cap, and the tip of the Twin Grasper 2 mm inside of the distal part of the cap, you release the clip.
Do not release the clip if your tip of Twin Grasper may still be outside or barely inside of the cap, as it may be entrapped by the OTSC
It is possible to close perforations up tp 30 mm with Twin Grasper and OTSC
can they be used to seal IBD related perforations
and fistulae?
This Live Chat on OTSC has been a success. Soon it will be available as an "article" for you to review. In addition, we have three lectures coming up during the EndoCollab Post-Graduate Course. I guarantee that you'll enjoy the lectures as well, with videos showing closure of fistulae, bleeding cases, anchoring of fully-covered self expanding metal stents, using the "sandwich" technique to close gastrocolonic fistula, etc.
Yes, IBD fistula and perforations are amenable to closure with OTSC. In May there will be a lecture on OTSC for closure of fistulas and perforations
We want to thank you for your input, questions, and participation.
Billions of thanks for sharing your experience and expertise
Looking forward to have more of such discussions
Looking forward to have more of such discussions
Thank you so much for joining! The chat has ended. Have a wonderful weekend :)

Nice discussion, thanks to everyone.
Have a great weekend
For your teaching file
Save this article as a PDF
Drop your email and we'll open a print-ready version you can save as a PDF — and you'll start getting our weekly GI endoscopy newsletter.