GI Endoscopy · 7 min read
How would you remove this pedunculated polyp (Paris 0-Ip, Kudo IIIL)?

TECHNIQUE ARTICLE
Abstract
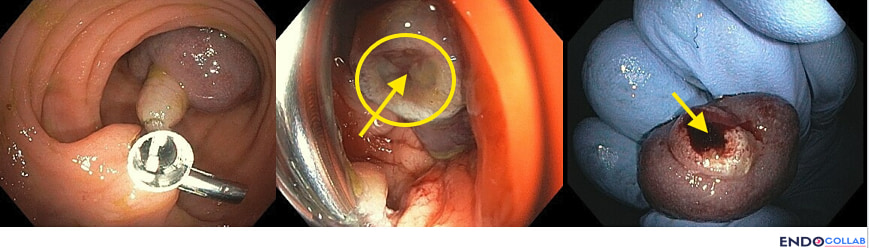
Background: Large pedunculated colonic polyps almost always carry a sizeable feeding artery within the stalk, and post-polypectomy bleeding can be brisk — particularly in patients on antiplatelet or anticoagulant therapy. Choosing how to secure the pedicle before transection is one of the most consequential decisions an endoscopist makes in this scenario. Approach: A 60-year-old man with hypertension, coronary artery disease, and atrial fibrillation on apixaban (held two days) presented with a large pedunculated polyp (Paris 0-Ip, Kudo IIIL) in the sigmoid colon. We placed two prophylactic hemoclips at the base of the stalk, then performed hot snare resection above the clips, proximal to the polyp head. Inspection of the resected pedicle revealed a prominent feeding vessel — confirming the value of pre-emptive hemostasis. Conclusion: For large pedunculated polyps, particularly in anticoagulated patients, securing the pedicle before transection — most commonly with hemoclips or an endoloop — is a low-cost, high-yield strategy that converts a potentially dramatic bleed into a controlled, predictable resection.Keywords: pedunculated polyp; Paris 0-Ip; Kudo IIIL; sigmoid polypectomy; prophylactic hemoclip; pedicle hemostasis; endoloop; underwater polypectomy; anticoagulation; post-polypectomy bleeding
Key Takeaways
- Every large pedunculated polyp should be assumed to have a substantial feeding vessel inside the stalk; the bigger the head and the thicker the pedicle, the bigger the artery.
- Secure the pedicle before you cut. Reactive hemostasis after a brisk arterial bleed is harder, messier, and far less safe than preemptive clipping or looping.
- In angled segments such as the sigmoid, hemoclips are usually more practical than endoloops; underwater resection adds a useful margin of safety by diluting any oozing and improving visualization.
- Risk-stratify by anticoagulation status. Patients on DOACs, warfarin, or dual antiplatelet therapy deserve a lower threshold for prophylactic mechanical hemostasis — even when the agent has been held.
- After resection, always inspect the stump and the specimen. The visible vessel in the pedicle is your confirmation that the prophylactic step was the right call.
Clinical Scenario
A 60-year-old man with a history of hypertension, coronary artery disease, and atrial fibrillation on apixaban (Eliquis) — held two days before the procedure — was referred for screening colonoscopy. In the sigmoid colon we encountered a large pedunculated polyp with a thick stalk and a prominent head. The lesion was classified as Paris 0-Ip with a Kudo IIIL surface pit pattern, consistent with a tubular or tubulovillous adenoma.Endoscopic Findings
The polyp measured roughly 25–30 mm at the head with a stalk of comparable thickness — a configuration that should immediately raise the suspicion of a sizeable feeding artery within the pedicle. Three features collectively predict a vessel of clinical importance:- A large polyp head — bigger heads need more blood flow for "nutrition," so the supplying artery scales accordingly.
- Advanced adenomatous features — neoplastic progression correlates with angioneogenesis; the more dysplastic the head, the richer the microcirculation.
- A thick stalk — the mechanical caliber of the pedicle directly tracks the caliber of the feeding vessel.
The Question
Before reading on, ask yourself: how would you resect this polyp?- Just snare
- Pre-injection and then snare
- Snare and then clip
- Pre-clipping and then snare
- Inject, clip, and snare
- Inject, snare, and then clip the stump
- Place an endoloop and then snare
- Snare and then place an endoloop
- Underwater snare resection
- Other
Discussion: Choosing the Approach
The honest answer is that all of these options can be correct — endoscopists have successfully removed pedunculated polyps every one of these ways. The real question is not whether a technique can work, but whether it gives you the safest, most predictable outcome for the patient in front of you. Many endoscopists prefer to cut first and then provide prophylactic or active hemostasis. That sequence is reasonable for small, thin-stalked polyps in low-risk patients. But it is genuinely risky in this scenario: post-resection bleeding from a thick pedicle can be brisk, especially in patients on anticoagulation or those with bleeding diatheses or dyscrasias. By the time you are scrambling to suction blood and identify the bleeding point, you are no longer in control of the field. I prefer to always perform prophylactic hemostasis BEFORE polyp resection in this setting. The most practical way to provide that prophylactic hemostasis is with hemoclips. (For a deeper look at clip selection and deployment mechanics, see our companion pieces on mastering the use of hemoclips and tips for placement of clips for hemostasis.) When available, endoloops are quite useful and equally safe — but placing a loop in angled positions such as the sigmoid colon can be challenging, and the loop has to sit at the right level on the stalk. A small pre-injection of saline, or saline with epinephrine 1:20,000, into the base can also help create a temporary tamponade and decrease blood flow to the polyp head. The trade-off is that injection can deform the stalk and make subsequent snare placement more awkward. Underwater or saline-submerged resection is another option I lean on increasingly; it offers two advantages: less thermal tissue damage during cutting, and dilution of any post-polypectomy bleeding with a clearer visual field. (We discuss underwater resection technique in cases such as endoscopic resection of a large duodenal lipoma and resection of a giant gastric polyp to treat upper GI bleeding.)Endoscopic Technique
In this case we opted for pre-clipping with two hemoclips, followed by hot snare resection above the clips, proximal to the polyp head.- Position the polyp at 6 o'clock in the field, with the stalk fully visualized. Adequate insufflation and a clean field matter — washing and suction first pays off.
- Deploy the first clip at the base of the pedicle, perpendicular to the stalk axis, capturing as much of the stalk thickness as the clip span allows.
- Deploy the second clip just adjacent to the first, slightly overlapping if needed, to ensure complete mechanical occlusion of the central vessel.
- Place the snare above the clips, leaving a small cuff of stalk tissue between the clips and the snare. This cuff protects the clips from being incorporated into the cautery cut and gives you a stump you can re-clip if needed.
- Resect using hot snare, with blended or pure-cut current per your institutional preference. Retrieve the specimen.
- Inspect the stump. If the clips are intact and the field is dry, you are done. If you see any oozing or a visible vessel, place an additional clip on the stump.
Practical Pearls
- For any pedunculated polyp with a head ≥10 mm or a thick stalk, default to prophylactic mechanical hemostasis — clips or loop — rather than reactive treatment.
- Two clips beat one. The central vessel can sit slightly off-center; doubling up improves your odds of complete occlusion.
- Always leave a tissue cuff between the prophylactic clips and the snare cut so you preserve a re-treatable stump.
- In a tough sigmoid angulation where you cannot get a loop seated, do not force it — use clips.
- Inspect the resected pedicle. The visible vessel is both your quality check and your teaching slide.
References
- Ferlitsch M, Hassan C, Bisschops R, et al. Colorectal polypectomy and endoscopic mucosal resection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline — Update 2024. Endoscopy. 2024;56(7):516–545.
- Kaltenbach T, Anderson JC, Burke CA, et al. Endoscopic Removal of Colorectal Lesions — Recommendations by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2020;158(4):1095–1129.
- Pohl H, Grimm IS, Moyer MT, et al. Clip Closure Prevents Bleeding After Endoscopic Resection of Large Colon Polyps in a Randomized Trial. Gastroenterology. 2019;157(4):977–984.
- Albéniz E, Álvarez MA, Espinós JC, et al. Clip Closure After Resection of Large Colorectal Lesions With Substantial Risk of Bleeding. Gastroenterology. 2019;157(5):1213–1221.
About the authors
For your teaching file
Save this article as a PDF
Drop your email and we'll open a print-ready version you can save as a PDF — and you'll start getting our weekly GI endoscopy newsletter.